An implantable device could enable injection-free control of diabetes
September 22, 2023
The device contains encapsulated cells that produce insulin, plus a tiny oxygen-producing factory that keeps the cells healthy.
Anne Trafton | MIT News
One promising approach to treating Type 1 diabetes is implanting pancreatic islet cells that can produce insulin when needed, which can free patients from giving themselves frequent insulin injections. However, one major obstacle to this approach is that once the cells are implanted, they eventually run out of oxygen and stop producing insulin.
To overcome that hurdle, MIT engineers have designed a new implantable device that not only carries hundreds of thousands of insulin-producing islet cells, but also has its own on-board oxygen factory, which generates oxygen by splitting water vapor found in the body.
The researchers showed that when implanted into diabetic mice, this device could keep the mice’s blood glucose levels stable for at least a month. The researchers now hope to create a larger version of the device, about the size of a stick of chewing gum, that could eventually be tested in people with Type 1 diabetes.
“You can think of this as a living medical device that is made from human cells that secrete insulin, along with an electronic life support-system. We’re excited by the progress so far, and we really are optimistic that this technology could end up helping patients,” says Daniel Anderson, a professor in MIT’s Department of Chemical Engineering, a core faculty member at the Institute for Medical Engineering and Science (IMES), a member of MIT’s Koch Institute for Integrative Cancer Research, and the senior author of the study.
While the researchers’ main focus is on diabetes treatment, they say that this kind of device could also be adapted to treat other diseases that require repeated delivery of therapeutic proteins.
MIT Research Scientist Siddharth Krishnan is the lead author of the paper, which appears today in the Proceedings of the National Academy of Sciences. The research team also includes several other researchers from MIT, including Robert Langer, the David H. Koch Institute Professor at MIT and a member of the Koch Institute, as well as researchers from Boston Children’s Hospital.
Replacing injections
Most patients with Type 1 diabetes have to monitor their blood glucose levels carefully and inject themselves with insulin at least once a day. However, this process doesn’t replicate the body’s natural ability to control blood glucose levels.
“The vast majority of diabetics that are insulin-dependent are injecting themselves with insulin, and doing their very best, but they do not have healthy blood sugar levels,” Anderson says. “If you look at their blood sugar levels, even for people that are very dedicated to being careful, they just can’t match what a living pancreas can do.”
A better alternative would be to transplant cells that produce insulin whenever they detect surges in the patient’s blood glucose levels. Some diabetes patients have received transplanted islet cells from human cadavers, which can achieve long-term control of diabetes; however, these patients have to take immunosuppressive drugs to prevent their body from rejecting the implanted cells.
More recently, researchers have shown similar success with islet cells derived from stem cells, but patients who receive those cells also need to take immunosuppressive drugs.
Another possibility, which could prevent the need for immunosuppressive drugs, is to encapsulate the transplanted cells within a flexible device that protects the cells from the immune system. However, finding a reliable oxygen supply for these encapsulated cells has proven challenging.
Some experimental devices, including one that has been tested in clinical trials, feature an oxygen chamber that can supply the cells, but this chamber needs to be reloaded periodically. Other researchers have developed implants that include chemical reagents that can generate oxygen, but these also run out eventually.
The MIT team took a different approach that could potentially generate oxygen indefinitely, by splitting water. This is done using a proton-exchange membrane — a technology originally deployed to generate hydrogen in fuel cells — located within the device. This membrane can split water vapor (found abundantly in the body) into hydrogen, which diffuses harmlessly away, and oxygen, which goes into a storage chamber that feeds the islet cells through a thin, oxygen-permeable membrane.
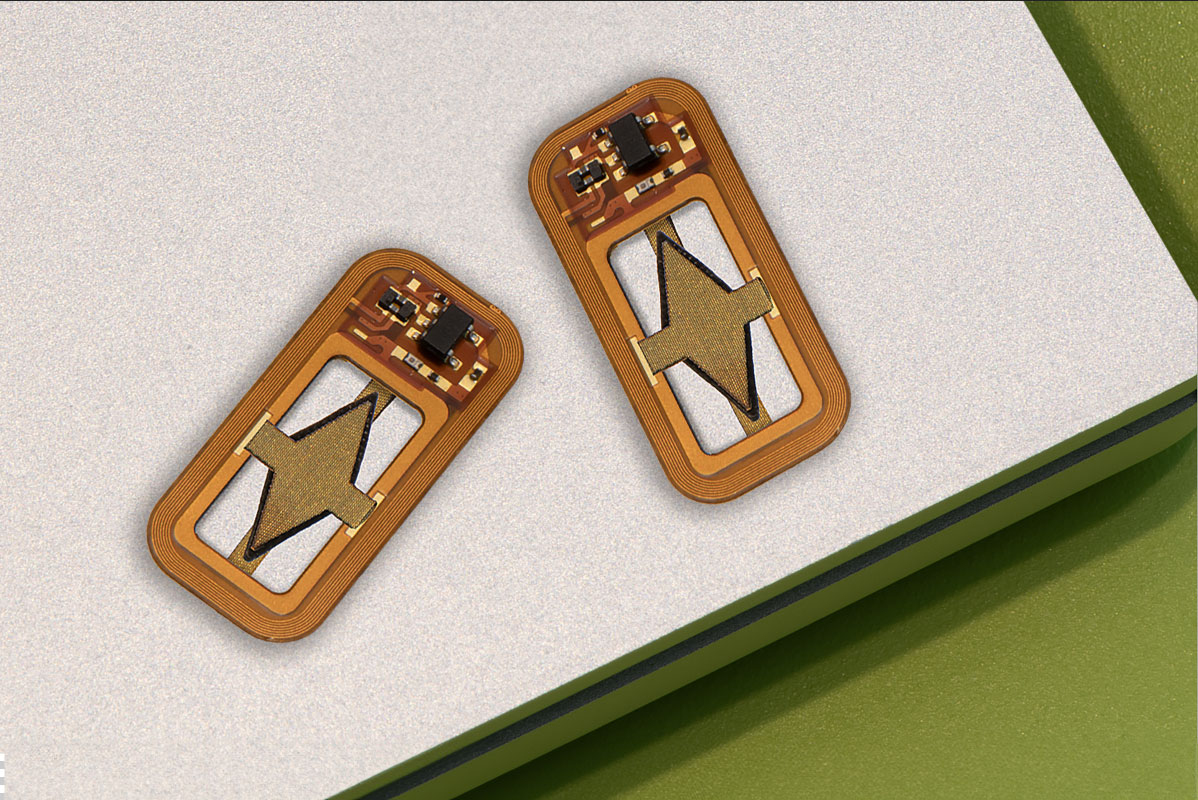
A significant advantage of this approach is that it does not require any wires or batteries. Splitting this water vapor requires a small voltage (about 2 volts), which is generated using a phenomenon known as resonant inductive coupling. A tuned magnetic coil located outside the body transmits power to a small, flexible antenna within the device, allowing for wireless power transfer. It does require an external coil, which the researchers anticipate could be worn as a patch on the patient’s skin.
Drugs on demand
After building their device, which is about the size of a U.S. quarter, the researchers tested it in diabetic mice. One group of mice received the device with the oxygen-generating, water-splitting membrane, while the other received a device that contained islet cells without any supplemental oxygen. The devices were implanted just under the skin, in mice with fully functional immune systems.
The researchers found that mice implanted with the oxygen-generating device were able to maintain normal blood glucose levels, comparable to healthy animals. However, mice that received the nonoxygenated device became hyperglycemic (with elevated blood sugar) within about two weeks.
Typically when any kind of medical device is implanted in the body, attack by the immune system leads to a buildup of scar tissue called fibrosis, which can reduce the devices’ effectiveness. This kind of scar tissue did form around the implants used in this study, but the device’s success in controlling blood glucose levels suggests that insulin was still able to diffuse out of the device, and glucose into it.
This approach could also be used to deliver cells that produce other types of therapeutic proteins that need to be given over long periods of time. In this study, the researchers showed that the device could also keep alive cells that produce erythropoietin, a protein that stimulates red blood cell production.
“We’re optimistic that it will be possible to make living medical devices that can reside in the body and produce drugs as needed,” Anderson says. “There are a variety of diseases where patients need to take proteins exogenously, sometimes very frequently. If we can replace the need for infusions every other week with a single implant that can act for a long time, I think that could really help a lot of patients.”
The researchers now plan to adapt the device for testing in larger animals and eventually humans. For human use, they hope to develop an implant that would be about the size of a stick of chewing gum. They also plan to test whether the device can remain in the body for longer periods of time.
“The materials we’ve used are inherently stable and long-lived, so I think that kind of long-term operation is within the realm of possibility, and that’s what we’re working on,” Krishnan says.
“We are very excited about these findings, which we believe could provide a whole new way of someday treating diabetes and possibly other diseases,” Langer adds.
The research was funded by JDRF, the Leona M. and Harry B. Helmsley Charitable Trust, and the National Institute of Biomedical Imaging and Bioengineering at the National Institutes of Health.
* Originally published in MIT News.